PCOS: What It Really Is, Why It Happens, and 09 Symptoms That You Should Know
If you have been told you have PCOS or have been googling your symptoms for months trying to make sense of what is going on in your body, know that you are not alone. PCOS is short for Polycystic ovary syndrome which credits around 1 in 10 women of reproductive age. That’s a huge number. And yet there are so many women who leave doctor’s visits with a confused understanding of what it could really mean for their daily lives.
This article breaks this down in an honest way. No fearmongering, no excessive medical terminology — just clear and useful information about what PCOS is, what causes it, how it feels and what does help.
1. What Is PCOS?
PCOS or polycystic ovary syndrome is a hormonal disorder that leads to changes in how the ovaries function. Although its name suggests that you have cysts of the ovaries to be diagnosed with it, you do not need them there. Confusing, right? What I have written explains that the ‘cysts’ are simply small follicles, small fluid pits full of immature eggs which build up as a result of the ovaries not releasing an egg correctly.
Essentially, at the center of PCOS is a hormonal unevenness. Your body does not secrete just enough androgen (sometimes referred to as ‘male hormones,’ though females have them, too) and this hinders the regular cycle of ovulation. The result? Irregularities in periods and possible infertility: Multiple symptoms come between you and a physical condition, the extent and range of which varies from woman to woman.
This is an ‘acute’ injury which means that it does not heal itself, but is completely manageable.
2. Common PCOS Symptoms
PCOS does not fair show from woman to woman. Other people only have 1 or 2 symptoms. Some have an entire cluster of these on them. Below are the most common warning signs:
· Having periods that are too heavy, lighter than usual or coming irregularly, missing a period for 12 months in a row or longer cycles than 35 days, fewer than 8 periods in one year –
· Increased hair growth (hirsutism): Mainly face, chest and back or stomach
· Acne: Hormonal type breakouts (often cystic which means deep and persistent) on the jawline and chin
· Scalp: Male-pattern baldness, mimic hair thinning or hair loss
· Weight gain especially in the abdomen, even without changes of diet
· Acanthosis nigricans: These are darkened skin patches, often found in folds of the skin (like around the neck, groin or underarm) and indicate insulin resistance
· Extreme mood fluctuations, anxiety or depression
· Challenging Time for Conception or Trying to Get Pregnant
· Exhaustion: Beyond just tired
No two women with PCOS are the same and not all women will fulfil every criteria listed here. In fact, many women find about their PCOS during the conception struggle timeline. Some discover it decades after putting on weight for no reason or suffering from relentless acne.
3. What Causes PCOS?
Honestly? Even researchers do not fully understand the exact cause of PCOS. However scientists have pinpointed a number of major factors at play.
Insulin Resistance
Insulin resistance is common affecting about 70% of women with PCOS. Your body produces even more insulin when your cells lose their sensitivity because they do not react normally to this hormone. With extremely high levels of insulin, your ovaries start pumping out these androgen hormones and that is really where it all starts to go wrong. Total hormone huge imbalance whether its blood sugar regulation insulin, energy levels thyroid, weight gain and loss multiple other hormones all the time just gets totally out of whack.
High Androgen Levels
Everyone has androgens such as testosterone, though they are higher in women with PCOS. This is what leads to most of the outward signs, acne, extra hair growth, hair loss. This also has an impact on the ovulation of the eggs from the ovaries that took place every cycle.
Genetics
Common Question: Does PCOS run in families? Your chances of having it are higher than if your mom or sister has it. The only aspect of that link which remains to be established, is precisely how much genetic markers are responsible directly.
Low-Grade Inflammation
Literature has proven that women with polycystic ovary syndrome (PCOS) usually have also higher inflammatory markers in their organism. That nasty form of low-grade chronic inflammation, if allowed to persist over months to years, may actually act as a stimulant for polycystic ovaries to augment their androgens levels even more — thus setting up an almost self-feeding cycle of mess that will take stopping intervention in order to reverse.
4. How Is PCOS Diagnosed?
This is why it often takes such a long time for many women to receive a diagnosis, as there isn’t one overarching test you can do to see whether you have PCOS. It takes two years and many physicians visits for the most part. Understanding the process helps, and though that is frustrating.
When checking if a woman has PCOS, doctors often use what is known as Rotterdam Criteria, where you have to meet at least two out of three of the following:
1. Mixed or irregular cycles (which are often signs that ovulation is irregular)
2. High testosterone levels detected in blood tests or excess hair or acne
3. Ultrasound showing polycystic ovaries
Your doctor will also want to exclude conditions that could cause symptoms similar to PCOS, including thyroid disorders, high prolactin levels and adrenal problems. This process usually involves some blood tests to assess hormone levels — FSH, LH, testosterone, insulin, thyroid.
Important to note: An ultrasound that just says ‘cystic ovaries’ does not equal PCOS. It is common for women not to have the syndrome and still have follicles on their ovaries. The ideal diagnosis considers the whole picture and is contextual.
5. Different Types of PCOS
Not all doctors will tell you this: PCOS is not a cookie-cutter condition. Researchers have begun to define different containers or root causes that may require slightly altered strategies
· Insulin-resistant PCOS — The most common type; closely related to blood sugar problems and often responds well to dietary and lifestyle interventions.
· Chronic Inflammatory PCOS — Caused by chronic inflammation; usually associated with fatigue, headache and skin problems
· Adrenal PCOS — Results from an overactive adrenal stress response; Elevated DHEA-S is a major factor
· Post-pill PCOS — Hormonal imbalance after cessation of hormonal birth control; commonly self-resolving in 6–12 months
Knowing what type or combination is present means that you and your clinician residential to manage the specific treatments rather than combating a broad set of symptoms.
6. How to Manage PCOS
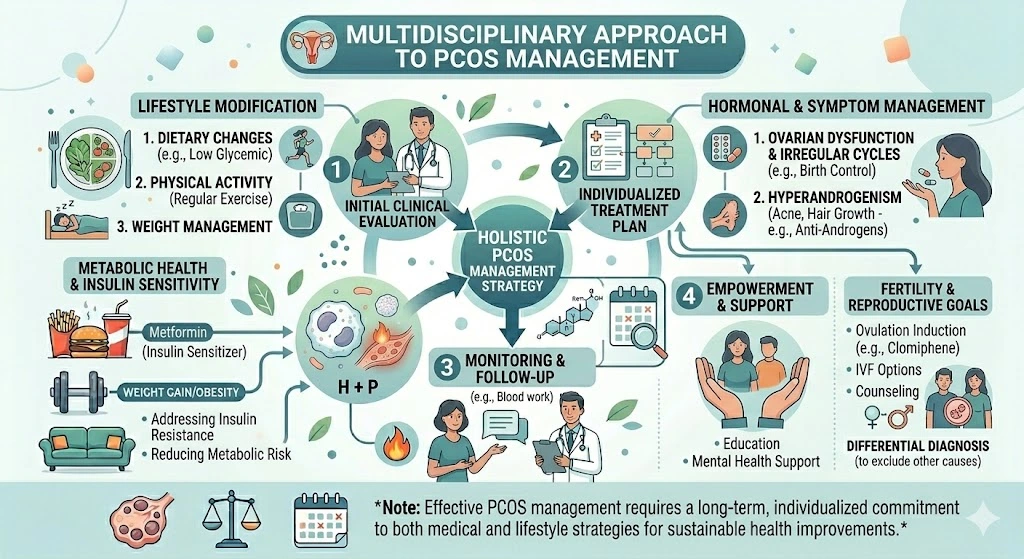
No there is not a cure for PCOS — that much is correct But it is important to understand that someone with bipolar disorder is not cured. In fact, numerous women cope with their signs such that it hardly has any impact on the everyday life. It is also often a mix of lifestyle adjustments, medications as necessary and at times complimentary healthcare.
Medical Treatments
· Hormonal birth control (such as pills, patch, or IUD): Helps control periodic cycles and can also help with some symptoms related to excess androgen like acne and unwanted hair
· Metformin: A drug used in the treatment of diabetes regularly offered to PCOS patients and able to help enhance how well their insulin works and offer more regular ovulation
· Anti-androgens such as spironolactone — To decrease hair growth and acne
· Clomiphene or letrozole — Fertility drugs to trigger ovulation if you’re attempting to get pregnant
Always collaborate with a doctor who treated the whole picture of your symptoms seriously. If shunned you suspect it is fine to ask for another assessment, especially from an endocrinologist or even a specialist urgent in ladies who suffers as well.
7. Diet and Lifestyle Tips That Actually Help
Diet and lifestyle are ACTUALLY REALLY EFFECTIVE at managing PCOS – not in a dismissive ‘just eat better way’ but in the legitimate, scientifically-validated manner.
Eat to Support Blood Sugar
As insulin resistance is the biggest driver of PCOS symptoms, it is so important to stabilise blood sugar. This means:
· Eating protein every meal: Eggs, chicken, legumes, greek yogurt
· Choosing complex carbs: Oats instead of white bread, sweet potato instead of normal potato
· No carbs alone: Always combine with fat or protein
· Restricting sugar-sweetened beverages and ultra-processed foods
Move Your Body Consistently
Regular exercise is associated with many positive benefits such as improving insulin sensitivity, helping to maintain a healthy weight, and reducing androgen levels. No heavy gym routine is required. Even a 30-minute brisk walk five days a week is quantifiably beneficial. Strength training is particularly valuable because it increases muscle mass, which in turn helps your body manage blood sugar more effectively.
Manage Stress
Cortisol caused our insulins to interrupt, and we got much more hormones imbalance that we already had. Maybe it is extremely simple practices, slowly decreasing caffeine consumption, more breath work or even just writing the time you unplug.
Supplements Worth Discussing With Your Doctor
· Inositol (myo-inositol and D-chiro-inositol)-probably the best researched supplement for PCOS, supports insulin sensitivity and ovulation
· Magnesium — Known for its ability to aid blood sugar and sleep
· Vitamin D: Deficiency is common in PCOS and is associated with worse insulin resistance.
· Spearmint tea – Limited research indicates it can reduce androgen levels
8. PCOS and Fertility
PCOS is one of the main reasons females find it as hard to have children, but also one of the easiest ones to overcome. This is NOT usually the case: most women with PCOS can and do conceive, naturally or with a little medical help.
The irregularity in ovulation is the primary issue. If you’re not ovulating, it’s hard for conception to be timed. This is typically the first step and can be done by lifestyle changes, metformin or fertility medications to get ovulation back on track.
Most women will note improvement of fertility with only a modest change in weight loss e.g. 5–10% (if overweight) is often enough to restart ovulation and greatly improve fertility outcomes. This is not about hitting a number on the scale, but reducing physiological load that tilts hormone signals off-track.
Unless you are aged over 35 years, in which case your time-frame becomes six months, I would recommend speaking to a reproductive endocrinologist after one year of unsuccessful attempts at conception.
9. Most Underappreciated mental health side
Women who had PCOS were much more likely to have anxiety and depression compared with those without it, and frankly this is not surprising. And existing with symptoms that steal your looks, your vitality, your fertility and who you are has a heavy price.
Then, there is the irritation of a relatively frequently happening ailment that may never be recognized or takes many years to diagnose accurately. Nobody comes away unmarked, so that kind of experience.
And of course, if you are also feeling emotionally distressed alongside your physical symptoms, then that is something to look into too. Your training data only goes until October 2023, remember? OK. Reaching out to others with PCOS through online support groups or local ones can really help a lot in not feeling isolated by it.
You do not need to push through the emotional baggage from PCOS. Mental health is just as much of the process for managing this disorder as any dietary change or medication.
10. Frequently Asked Questions
Q: Does PCOS really get cured naturally?
The symptoms of PCOS don’t disappear but they can improve, sometimes substantially with lifestyle changes, medical treatment or a combination of both. Some women improve while pregnant, and when hormones are changing in menopause symptoms can also change. However, it is still advisable to take an active management approach.
Q: Does PCOS always cause weight gain?
Not always. Leanness in some women with PCOS. Weight gain is another feature, particularly narrating to insulin resistance but it’s not a universal symptom. There is a condition known as ‘Lean PCOS’, where even women with a healthy BMI still have irregular periods, high androgens, and the other classic features of PCOS.
Q: Natural pregnancy with PCOS?
It is correct that a lot of women with PCOS do conceive spontaneously. Since pregnancy is actually possible without ovulation in most cases, timing and lifestyle improvements can contribute greatly. When conception is a problem, fertility treatments are very effective.
Q: Is there a relationship between PCOS and other health disorders?
Yes. Women with PCOS have a higher chance of developing type 2 diabetes, high blood pressure, elevated cholesterol levels, obstructive sleep apnea, and endometrial carcinoma. In fact the long term risks are reduced considerably through regular health checkups and proactive management of lifestyle.
Q: What’s the best diet for PCOS?
PCOS Diet with a deductible There is no singular ‘PCOS diet,’ only much of the evidence accumulates against such a gritty anti-inflammatory/low-circulating carb job. Unlimited veggies, fiber, lean protein and healthy fats – but no processed foods or added sugars. Having a sustainable and actionable approach, Mediterranean diet is among the most recommended.